AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2640-1053/023
1 Department of Orthopaedic Surgery, India
*Corresponding Author: Sakthivel Rajan Rajaram Manoharan, Department of Orthopaedic Surgery, India
Citation: Sakthivel Rajan Rajaram Manoharan, Feasibility of cognitive sparing approaches in children with intracranial tumors requiring partial brain radiotherapy: A dosimetric study using tomotherapy .J Cancer Research and Cellular Therapeutics, Doi: 10.31579/2640-1053/023
Copyright: © 2018 Sakthivel Rajan Rajaram Manoharan . This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 05 January 2018 | Accepted: 20 February 2018 | Published: 26 March 2018
Keywords: cognitive sparing; intracranial tumors; brain radiotherapy
Background: To assess feasibility of sparing the neural stem cell compartment (NSC), hippocampus, and limbic circuit during partial brain radiotherapy (PBRT) for pediatric intracranial tumors.
Methods : Treatment plans were generated for the following pediatric intracranial tumors: low and high grade gliomas, low grade brainstem glioma, optic nerve glioma, hypothalamic glioma, localized ependymoma, skull base sarcoma, central nervous system (CNS) germinoma (involved field radiotherapy [IFRT] and whole ventricular radiotherapy [WVRT] ), and craniopharyngioma. For each pathology, standard intensity-modulated radiotherapy (IMRT) plans were generated using helical tomotherapy, as well as IMRT plans which spared limbic circuit, hippocampus, and NSC. Biologically equivalent dose for late effects (BEDlate effects) was generated for limbic circuit, hippocampus, and NSC. Percent reduction in mean, maximum, and minimum physical dose and BED was calculated between plans.
Results: We reduced mean physical dose and BEDlate effects to these critical structures by 44% and 47.9% respectively (range 5.4-78.8% and 7-80.3%). Greatest benefits in relative dose reduction were seen in high grade hemispheric glioma cases; least relative dose reduction was seen in WVRT cases. Dosimetric coverage of treatment target (PTV) was equivalent in all cases as assessed by D95 and V100 metrics. Integral dose to uninvolved brain was reduced by mean of 7.6% (range -19.3% to +0.3%) in sparing plans.
Conclusions: It is possible to spare limbic circuit, NSC, and hippocampus during PBRT for primary pediatric intracranial tumors using helical tomotherapy. This approach reduces integral dose delivered to uninvolved normal brain and may reduce late cognitive sequelae of cranial radiotherapy.
Cranial irradiation plays a role in the treatment of many different primary pediatric intracranial tumors. [1-10] However, the role of radiotherapy in this setting has been gradually diminishing based largely on concerns over the late adverse consequences of cranial irradiation.[11-15] These late effects include cognitive dysfunction, endocrinologic dysfunction, and cerebrovascular morbidity. [13-15] Many of the late adverse cognitive consequences of cranial irradiation may relate to damage to the neural stem cell compartment (NSC), limbic circuit (LC), and hippocampus. [16-18 Sparing of these critical structures dosimetrically may reduce the incidence and/or severity of late adverse cognitive sequelae in treated patients . [17-18] Our group has shown that it is dosimetrically feasible to spare these regions in the setting of whole brain radiotherapy (WBRT), prophylactic cranial irradiation(PCI) and partial brain radiotherapy for adult low and high grade gliomas. [19-21] In this study we demonstrate the feasibility of sparing these structures in the setting of PBRT using common treatment fields and dosing schedules for a number of different primary pediatric intracranial tumors This strategy should reduce the late adverse effects of cranial irradiation for this group of patients.
We selected one representative pediatric patient treated in our department within the past 4 years (2007-2010) with each of the following diagnoses: low grade supratentorial hemispheric glioma, high grade supratentorial hemispheric glioma, low grade brainstem glioma (biopsy-proven WHO grade 1 astrocytoma of the midbrain), right optic nerve glioma, suprasellar CNS germ cell tumor, high grade chondrosarcoma of the right sphenoid bone, suprasellar craniopharyngioma, infratentorial ependymoma (without leptomeningeal dissemination), and low grade glioma (WHO grade 1) of the infindibular stalk. Two intensity modulated radiotherapy (IMRT) treatment plans were prepared for each patient using helical tomotherapy (TomoTherapy@, Madison, Wisconsin): one plan (STD: standard) which did not apply optimization criteria to the limbic circuit (LC), hippocampus (HIP), or neural stem cell compartment (NSC), and another plan (SPA: sparing) which attempted to minimize the maximum and mean doses to these same structures For each patient, an appropriate treatment target (PTV: planning target volume) was contoured, and this PTV was applied both the STD and SPA plans. The PTV varied by diagnosis, but generally consisted of the gross tumor as identified on imaging, areas of edema or areas otherwise felt to be at risk for containing microscopic tumor (for example, the ventricular system plus a 1cm margin for CNS germinoma whole ventricular radiotherapy plans), and an additional margin for setup uncertainity on the treatment table.
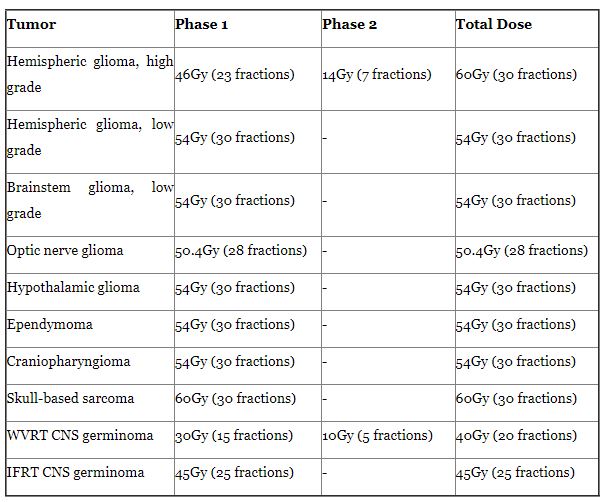
Adequate target coverage, as defined by the D95 (isodose line covering 95% of the PTV) and V100 (percent volume of the PTV receiving at least full dose/100% of the planned treatment dose), was required as the primary treatment objective in all plans (STD and SPA). The dose prescriptions/ treatment schedules for each plan type are shown in (Table 1). Also, standard constraints were applied to the following critical normal structures (OAR: organs at risk) in all plans (STD and SPA): right and left lenses, right and left eyes, right and left optic nerves, optic chiasm, pituitary/infindibulum/ hypothalamus, right and left cochleae, brainstem, and spinal cord. These standard OAR dose constraints are shown in (Table 2)

For the SPA plans, we provided additional optimization criteria to maximally spare the study OAR (LC, HIP, and NSC) by placing restrictions on the mean and maximum doses to these structures (third priority). These study OAR were spared contralaterally for the supratentorial hemispheric low and high grade glioma and skull base sarcoma plans, and bilaterally for the other plans.
For each plan the physical doses and biological equivalent doses (BED) delivered to the following structures were calculated: PTV (D95, V100, minimum dose, and maximum dose) and study OAR (LC, HIP, and NSC: meandose, maximum dose, and minimum dose). Within each tumor subgroup, delivered physical dose and BED to the PTV and study OAR were compared between the STD and SPA plans, and percent relative differences were calculated. The physical doses delivered to the standard OAR (right and left lenses, right and left eyes, right and left optic nerves, optic chiasm, pituitary/infindibulum/hypothalamus, right and left cochleae, brainstem, and spinal cord) were evaluated for each plan (STD and SPA) to ensure that they did not exceed our acceptance criteria (Table 2), but BED were not calculated and the dose delivered to these structures were not compared between the STD and SPA plans. The BED, which represents a measure of the biologic likelihood of a given dose of radiation delivered on a given treatment schedule causing a given effect on a given tissue type (tumor or normal structure) for each of these structures was calculated using the following equation, where n is the number of fractions and d is the dose per fraction in Gy:
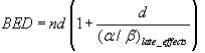
We assumed an alpha/beta (α/β) ratio of 2 for late effects involving LC and HIP. For PTV and NSC we conservatively assumed an α/β ratio of 10 because it is a value previously demonstrated for other tumors and stem cell populations [22]. The α/β ratio represents the ability of a given cellular type to repair sublethal damage to its DNA generated by radiation exposure, and is generally low (around 2-3) for tissues with little or no cellular turnover (and thus plenty of time available to repair damage before the next mitosis) such as muscle cells, fibroblasts, and neurons. The α/β ratio is high (around 10) for cells which are proliferating quickly and thus have little time available for DNA repair between mitoses, such as skin, gut epithelial cells, stem cell populations, and most tumors. No such studies have been completed for human NSC in vivo, and therefore our choice of an α/β ratio of 10 for this cellular population remains speculative.
Since this is a dosimetric comparison study we investigated whether the SPA plans increase the integral dose to the normal uninvolved brain versus the STD plans. Integral dose, expressed in joules (J), represents the total energy deposited in a given mass of tissue, and is generally represented by multiplying the delivered dose (in Gray, or joules/kg of tissue) by the mass of tissue exposed (in kg). For each plan, OAR's designated as "uninvolved brain" which contained all brain parenchyma not otherwise included in standard OAR, study OAR, or treatment targets (PTV) were generated, The integral dose, ID, was computed from differential dose volume histograms using the following equation:

is the average physical density of the uninvolved brain, Vi is the volume in m3 of each dose voxel and Di is the dose, in Gy, in each voxel. All is the average physical density of the uninvolved brain, Vi is the volume in m3 of each dose voxel and Di is the dose, in Gy, in each voxel. All these values are easily extracted from dose volume histograms. Using an average density instead of a voxel specific density in Equation 2 is warranted since the brain density is rather uniform, which is not the case in highly heterogeneous regions such as lung. The integral dose can be expressed as a single value or as a dose-ID histogram d-IDh.
Dosimetric coverage of the treatment target (PTV) was excellent in all STD and SPA plans, with 94.8-96% of PTV receiving full dose in STD plans and 4.9-95% receiving full dose in SPA plans. However, there was greater dose inhomogeniety noted in the SPA plans, with minimum doses 56 to 99% (mean 90%) and maximum doses 101 to 128% (mean 109%) of prescription dose. The corresponding ranges for the STD plans were to 81 to 99% (mean 92%) minimum doses and 101 to 120% (mean 105%) maximum doses relative to the prescription dose. All plans (STD and SPA) were able to meet the dose constraints for all standards OAR as described in (Table 2) (individual plan data not shown).
SPA plans were able to significantly reduce mean physical dose and BED delivered to the study OAR (LC, HIP, and NSC) in all cases: percent reduction in mean physical dose 5.4 to 78.8 (mean 44) and percent reduction in mean BED 7 to 81.5 (mean 47.9). The corresponding percent reduction in mean physical dose and BED for the limbic circuit, hippocampus, and neural stem cell compartment were 5.4 to 77.8 (mean 43.3) and 7 to 80.3 (mean 47.2), 18.2 to 67.4 (mean 46.5) and 25.4 to 81.5 (mean 52.4), and 6.8 to 60 (mean 42.1) and 7.8 to 66.1 (mean 44.1), respectively. In most cases the minimum and maximum physical doses and BED delivered to the study OAR were also reduced in the SPA, although in a some cases the minimum physical dose and BED were higher (craniopharygioma and optic nerve glioma plans: LC absolute minimum physical dose increased by .05 to .1 Gy, mean 0.8 Gy) while in others the maximum physical dose and BED were higher (IFRT, WVRT, high grade glioma, low grade glioma, and craniopharyngioma plans: absolute maximum physical dose increased by .63 to 8.6 Gy, mean 2.5 Gy) for the SPA plan despite a lower mean physical dose and BED, evidence of greater dose inhomogeneity within the study OAR for the SPA plans.
Integral dose (J) delivered to the uninvolved brain was reduced in the SPA plans as compared to the STD plans by a mean of 7.6% (range -19.3% to +0.3%). The greatest reduction in integral dose was noted in the high grade glioma SPA plans (19.3% reduction), The only treatment plan type in which integral dose was increased with sparing techniques was WVRT (0.3% increase in SPA plan versus STD plan) only treatment plan type in which integral dose was increased with sparing techniques was WVRT (0.3% ncrease in SPA plan versus STD plan).
Cranial radiotherapy plays an important role in the treatment of a number of primary pediatric intracranial tumors [1-5]. In the case of CNS germinoma and brainstem glioma, cranial radiotherapy is a standard primary treatment modality, and studies in the setting of CNS germinoma which have attempted to exclude radiotherapy as a component of treatment have shown significantly inferior results [6-8,10].
Unfortunately, the use of cranial radiotherapy in children results in a number of adverse late sequelae include cognitive dysfunction, endocrinologic dysfunction, and vascular damage [13-15]. The cognitive dysfunction can be profound, with St. Jude Children's Hospital and others finding a direct correlation between the dose administered and a decline in overall IQ [14,23-26]. In the St. Jude study, the factors that seem to correlate most strongly were younger age at time of treatment, longer time interval since treatment, female sex, presence of hydrocephalus, higher volume of supratentorial brain irradiated, and higher radiation dose to the supratentorial brain [26]. They also found that irradiation of the supratentorial compartment and temporal lobes resulted in significant declines in IQ regardless of the dose exposure, with each Gy of exposure having a similar impact on declines in IQ [23]. The cognitive deficits seen after treatment are predominantly the inability to develop new skills and process new information, rather than loss of previously acquired function and memories [14].
Changes in fractional anisotropy (FA) on diffusion tensor imaging (DTI) MRI provide evidence of damage to white matter pathways, and these changes can be seen in pediatric patients who have been treated with radiotherapy for medulloblastoma and surgical resection for cerebellar astrocytomas, with one recent study showing a mean reduction in FA of 16.5%in treated patients versus controls [27-29]. These reductions in FA were found to correlate with a younger age at the time of treatment and declines in school performance [28]. Rueckriegel et al. found that supratentorial changes in FA were more prominent in patients treated with radiotherapy and surgical resection than with surgery alone, although the distribution of deficits was similar. Interestingly, the location of most of the changes as identified in (Figure:1 & 2) of their paper lie within the hippocampus, limbic circuit, or neural stem cell compartment [29].


Johannesen and colleagues have shown in a retrospective review of MRI studies from a group of adult patients previously treated with cranial radiotherapy (median dose 54 Gy) that doses of 29.2 Gy or above are associated with grade 3 white matter changes on MRI T2 and FLAIR sequences and worse neurocognitive outcomes and patient-reported quality of life, while doses in the range of 12.5-27.5 Gy delivered to the contralateral hemisphere were not associated with such changes [30]. This study, although performed in adult patients, is consistent with the findings from the group at St. Jude's which found that the percent volume of pediatric supratentorial brain irradiated to varying dose levels (0-20Gy, 20-40Gy, 40-65Gy) correlated with IQ level after cranial irradiation [24].
Since the total dose delivered to the brain in the treatment of primary pediatric brain tumors exceeds this threshold of 20-27.5Gy (Table 1:), it would follow that reduction of dose to non-target regions of the brain in children should improve imaging and clinical outcomes [29-30].
Several investigators have demonstrated the feasibility of sparing NSC, limbic circuit, and/or hippocampus in adults during the administration of partial brain radiotherapy (PBRT) for glioma and whole brain radiotherapy (WBRT) [19,21,32-34]. The Radiation Therapy Oncology Group (RTOG) is currently accruing patients to a phase II study (RTOG 0933) which aims to demonstrate the feasibility of sparing the hippocampus during the administration of whole brain radiotherapy. This study will incorporate baseline and follow up neurocognitive testing to assess the impact of hippocampal sparing on memory and other cognitive domains after treatment [RTOG.org].
Cranial irradiation also produces damage to the hypothalamicpituitary axis, particularly in children at doses as low as 18Gy [13,35-38]. This study was not designed to specifically evaluate dosimetric sparing of the pituitary-hypothalamic axis, but we are able in all plans (STA and SPA) to meet our planning objectives for the hypothalamic-pituitary axis.
Thus, efforts directed toward dosimetrically sparing the study OAR did not compromise dosage to the pituitary-hypothalamic axis.
In the current study, we have demonstrated the feasibility of sparing the limbic circuit, hippocampus, and neural stem cell compartment, with mean physical dose and BED to each structure reduced 44% and 47.9%, respectively. In most cases we selected these structures bilaterally for sparing, but in the hemispheric glioma and skull base sarcoma plans we elected to spare these structures contralaterally as they could not be spared ipsilaterally due to the proximity of the PTV to the ipsilateral study OAR. We anticipate that these patients (those with the study OAR spared contralaterally only) will still derive a late cognitive benefit based on the available literature detailing the cognitive outcomes for patients who have undergone surgical temporal lobectomy for treatment of tumor or intractable epilepsy [40-42]. Such patients rarely have persistent cognitive deficits provided that the resected medial temporal lobe structures are diseased and the remaining medial temporal lobe structures are normal, suggesting that the remaining structures can compensate for any transient deficits sustained from the surgical procedure [40-42].
We believe that damage to the critical study OAR in this study (LC, HIP, NSC) is the principal cause of late neurocognitive deficits in both adult and pediatric patients, and our sparing is based around this assumption. However, others have suggested that low dose radiation exposure to the whole brain produces (or at least contributes) to these late adverse effects [43-44]. This theory suggests that it is reduction of the integral/overall dose to the brain which will ultimately provide cognitive protection. Investigators from Brazil has demonstrated the ability of IMRT to reduce the high dose regions and integral dose to the brain during the delivery of WVRT for primary CNS germinoma [31]. We similarly found in this study that the use of Tomotherapy IMRT reduced the integral dose delivered to the uninvolved brain by a mean of 7.6%, with all plan types showing benefit except for the WVRT plans, in which sparing techniques increased integral dose by 0.3%. This reduction in integral dose to uninvolved brain might also reduce the incidence of secondary tumor induction in this at-risk patient population.
Recently concern has been expressed over the use of intensity-modulated radiotherapy (IMRT) in the setting or cranial irradiation, since more total monitor units (MU) are required to deliver a given dose with this treatment modality, resulting in greater integral dose being delivered to the patient [45-47]. This finding has been shown in some but not all dosimetric studies comparing IMRT to either conventional/2-D or 3-D conformal treatment planning, with some studies showing a higher ID delivered to the brain and other showing a lower ID[45-51]. Reduction of ID should, in theory, reduce the risk of late second malignancies and cognitive dysfunction, although this has not been conclusively proven [45-46].
IMRT also produces more inhomogeneous dose distributions than conventional or 3-D conformal radiotherapy plans, with greater hot and cold spots (areas receiving greater than and less than prescription dose, respectively). This issue was noted in our treatment planning study, in which hot spots within the PTVs were in some cases >120% of presecription dose. While ideally these hot spots will be positioned within the tumor rather than within normal tissue, there is some concern that hot spots in normal brain may increase the risk for late adverse effects such as radionecrosis. For example, the commonly accepted TD5/5 (the dose which will result in a 5% risk of adverse events at 5 years in a given tissue) for normal partial brain is 60Gy [52]. Therefore, in the context of IMRT treatment planning for intracranial malignancies it would be prudent to minimize hot spots to the extent possible, and if possible to have them located within tumor rather than normal brain.
Also, since most recurrences of glioma (high and low grade) occur at or within 2cm of the original site of disease after resection and/or radiotherapy, we do not believe that our cognitive sparing approach will increase the risk of relapse for these patients, as we did not compromise definition or dosimetric coverage of our treatment targets (Table 1: and el) [56].
Another important approach to normal tissue sparing in the setting of cranial radiotherapy for pediatric brain tumors is the use of proton therapy [57-69]. Investigators at several institutions have performed dosimetric studies comparing the dose delivered to normal tissues with proton therapy as compared to IMRT and/ or conventional radiotherapy, and have consistently shown a reduction in dose to critical normal tissues favoring proton therapy [57,60,64-65]. Proton therapy has also been shown to reduce the integral dose to the body when compared with IMRT, and this reduction in integral dose is expected to result in a lower rate of secondary tumor induction after treatment [66-69]. This is a particularly important issue in children, and the use of IMRT (including helical tomotherapy) in this context, with its associated higher total body integral dose (due to a higher number of monitor units [MU] and higher leakage dose required to deliver a given dose of therapeutic radiation), should be approached with caution [67-68]. Importantly, no prospective randomized trials have been performed comparing proton therapy versus IMRT clinical outcomes in terms of either tumor control or late effects in the setting of adult or pediatric primary tumor treatment.
We believe that the cognitive sparing approach detailed in this study and our previous studies should be implemented in the setting of a prospective clinical trial [19,21,39]. Formal neurocognitive data should be collected at baseline and following treatment to assess the functional outcome for these patients, and these results should be compared with those of either a control group treated prospectively without this approach or a historical control group with adequate follow up and neurocognitive data outcomes. Without such data, it will not be possible to properly assess the relative benefits of our approach.
It is dosimetrically possible to reduce physical dose and implicitly BED to the limbic circuit, hippocampus, and neural stem cell compartment during the administration of partial brain radiotherapy for the treatment of multiple types of pediatric primary intracranial tumors. Such treatment does not compromise dosimetric coverage of the treatment target or compromise dosimetric sparing of other critical normal structures including the pituitary-hypothalamic axis. Our cognitive sparing approach reduces integral dose to normal when compared to standard approaches in most cases, and should reduce the late adverse cognitive effects of radiotherapy in children, but needs to be studied in the context of a prospective clinical trial with formal evaluation of neurocognitive outcomes.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
